
CARLSBAD, CA (October 17, 2017) – The San Diego County Medical Society (SDCMS) has worked collaboratively with San Diego Magazine for more than 10 years to recognize physicians who are held in the highest regard by their peers. Many of the nominees have been recognized for multiple years since the award began.
The NextMed Center of Carlsbad is pleased to announce that the following physicians have been selected to receive the prestigious San Diego Magazine Top Doctor Award for 2017:
REPRODUCTIVE ENDOCRINOLOGY/INFERTILITY:
• Arlene Joan Morales, MD****
Fertility Specialists Medical Group

OBSTETRICS AND GYNECOLOGY:
• Kim M. Goodwin, MD********
West Coast OB/GYN Associates
• Craig Sean Saffer, MD*******
West Coast OB/GYN Associates
• Lauren Denise Bales, MD**
West Coast OB/GYN Associates
• Amy Colleen French, MD**
West Coast OB/GYN Associates
• Daniela S Meshkat, MD***
West Coast OB/GYN Associates
• Christina Maria Chirico, MD*
West Coast OB/GYN Associates
GENERAL SURGERY:
• Adam Samuel Fierer, MD******
Minimally Invasive Surgeons of North County

Note: * denotes number of years the doctor has been nominated on the list.
The NextMed Center of Carlsbad medical campus is the hub for innovative medical treatments with an eye to defining the future of medicine.
From women’s services to regenerative medicine; orthopedics to same-day surgery – the best doctors in the country have come together to serve patients in the beautiful seaside town of Carlsbad.
SAN DIEGO, California, May 18, 2017 (eReleases)-
After suffering a potentially career ending knee injury, Brian Farber of the San Diego Sockers in the Professional Arena Soccer League searched for a treatment to get him back in the game. After a few failed attempts, Farber turned to stem cell therapy. He would later become one of the first people in San Diego to receive this innovative regenerative medicine treatment.
Farber had suffered a knee injury and torn patellar ligament about two and a half years earlier. Initial treatment with physical therapy and platelet rich plasma injections were unsuccessful. He was not a candidate for surgery and was told that he would “just have to live with the pain”. But, the pain made it difficult to resume professional soccer and his other favorite daily activities such as jogging with his wife and teaching at his soccer academy. Farber had even considered retiring from professional soccer.
Fortunately, a colleague introduced him to Dr. Christopher Rogers, founder of the San Diego Orthobiologics Medical Group. Dr. Rogers had treated many other patients successfully and was confident that stem cell therapy would heal Farber’s injury. Dr. Rogers is the first physician in San Diego to offer this state- of-the-art and FDA compliant treatment known as Lipogems®. The safety and efficacy of this new technology has been validated by several research studies.
This was the information Farber needed to take a chance with stem cell therapy. The Lipogems® procedure involves the use of liposuction to harness a patient’s own fat derived stem cells. Dr. Rogers uses high resolution ultrasound imaging to visualize the injury and to inject stem cells into the injured tissue. Farber decreased his activity for ten days to facilitate the healing process. Follow-up care included physical therapy, progressive strengthening and BEMER technology, which uses pulsed electromagnetic waves to stimulate cellular activity and improve circulation. Farber’s hard work and Dr. Roger’s expertise paid off. Within three months Farber was feeling strong and by six months he was playing competitive soccer without any pain.
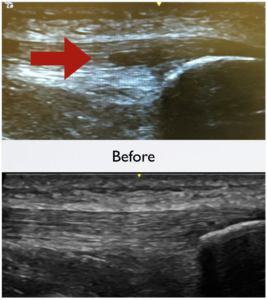 The patellar tendon is healed 3 months after treatment with Lipogems®.
The patellar tendon is healed 3 months after treatment with Lipogems®.
Farber, who is known to his soccer fans as “Flash” is pleased that he can stand up to his nickname once again. He says that “it feels great to run without pain”. He was recently voted Comeback Player of the Year and selected to the Indoor National Team. He is preparing for the Indoor World Cup which would not have been possible had he remained injured.
Dr. Rogers and his team at the San Diego Orthobiologics Medical Group are proud to have helped Brian achieve such a high level of performance and we will be rooting for Brian and the San Diego Sockers this year.
For more information regarding the San Diego Orthobiologics Medical Group stem cell therapy, please visit: http://www.sdomg.com
November 28, 2016
Kristi Maas, MD, ME, FACOG
Who me?
If you are reading this, chances are you are someone who may be interested in having children at some point in your life. You may not necessarily be at that point today- you may never reach that point- but don’t set this article aside; it is intended for you! Now is the best time inform yourself, consider your options, and take action if you want to!
Deciding when or if you want to get pregnant
As women we have competing interests with respect to our fertility. We desire to prevent pregnancy until a time we feel ready, but we also want to easily become pregnant when we are ready. The introduction of birth control pills in the 1950s and their widespread availability have allowed women to prevent unwanted pregnancies and better time a pregnancy for their life schedule. This trend, in combination with a shift towards women entering careers outside of the home, has resulted in women being older at the time of giving birth to their first child.
According to the Centers for Disease Control in 1970 the average age at first birth was 21.4 years and it increased to 25.8 years in 2012.[1] The rise reflects a six-fold increase in the number of first time mothers aged 35-39 and a four-fold increase among mothers 40-44 years old.[1]
With advancing age at first born, more women are faced with infertility. After many years of hiding these struggles due to fear or shame, patients with infertility are finally sharing their stories and the problem is well recognized. With this recognition comes a call for action. Women are motivated to prevent this difficult diagnosis.
How many eggs do you have and can you get more?
Our current understanding of female fertility is that a woman’s egg supply is a fixed pool of eggs that develop while a woman is still in her mother’s womb. This egg supply peaks at 6-7 million when she is approximately 20 weeks of gestation for her mother. The pool of eggs declines over time and at birth it is approximately 1-2 million.
A woman’s eggs remain in a resting state until she reaches puberty at which time she will start to develop multiple follicles with eggs every month. A primary follicle is selected from those that are developing and the other follicles die off. This primary follicle is the one from which a woman ovulates (releases a single egg). As a result, a woman uses up more than one egg per month despite generally only having one egg released and available to create a baby.
How does an egg become a baby?
When the egg is released from the ovary it is swept into the fallopian tube where it can meet with sperm to create an embryo. The embryo then travels down the fallopian tube and implants in the uterus. In an uncomplicated pregnancy, forty weeks later, a baby is born.
Why your age matters
If a woman is born with all of the eggs she will ever have and these eggs are lost over time it is clear that time and, therefore, age play an important role in fertility. In addition to a decreased supply, the remaining eggs from older women are more likely to be chromosomally abnormal as her age increases. Chromosomes contain genetic material that is passed from a parent to a child and chromosomally abnormal pregnancies are less likely to lead to a live birth. It is estimated that approximately 5% of a 25 year old woman’s eggs are chromosomally abnormal whereas 10-25% are abnormal among women in their thirties.[2,3,4,5] This number rises significantly to 50% or higher for women in their forties.[2,3,4,5] The increasing rate of abnormalities is due to the process of egg maturation and development prior to fertilization with sperm.
What can affect your ovaries and how well they work?
Genetic conditions such as Fragile X Syndrome and Turner’s Syndrome (45X0) are known to be associated with loss of egg number and quality at younger ages. Eggs can also be injured or prematurely depleted by treatments termed “gonadotoxic.” Gonadotoxic therapies include select medications such as chemotherapy, radiation, surgery to the ovaries or the blood supply to the ovary, or significant long-term health conditions.
When a woman faces a diagnosis of a serious chronic medical condition, cancer, or the need for gynecologic surgery she should be counseled about the reproductive risks of her disease and/or treatment. We know that radiation and chemotherapy are gonadotoxic, meaning they injure the ovaries and eggs, and that the effects depend upon the amount of the gonadotoxin and the age of the woman when she is treated. As a woman’s age at treatment increases relatively smaller doses of the gonadotoxin will result in a more significant loss of egg number and/or quality.
The treatment of pediatric, adolescent, and young adult cancers has become more effective and survivors have longer life expectancies. This underscores the need for discussion of the effects of therapy on fertility and the preservation of fertility prior to treatment.
Can we preserve fertility?
Previously, many women facing gonadotoxic therapy were given neither information nor the option to undergo fertility preservation. When the information was provided the only available method to preserve female fertility was to freeze embryos. This created a significant dilemma for single women, lesbians, bisexuals, or women not in a committed relationship with someone whom they can or would like to use their sperm to create embryos. The introduction of egg freezing now allows women to preserve their fertility independently.
The use and success of egg freezing in patients facing gonadotoxic therapies has opened the door to fertility preservation for women who desire to delay childbearing for personal or professional reasons. Many women find this an empowering option, allowing them to essentially stop their biological clock and taking the pressure off of creating a family “before it’s too late.”
How to choose when to preserve your fertility?
Regardless of the reason a woman decides to preserve her fertility, the best time to do it is now. It is clear that fertility declines with age and it is impossible to know how long a woman’s fertility will remain functional. Each woman’s fertile window- the time where she is able to become pregnant naturally- is different. The window is affected by multiple factors including health, family history, exposure to gonadotoxins, and even other currently unknown factors. At this time, closure a woman’s fertile window can’t reliably be predicted.
Can you find out how well your ovaries will respond?
Despite the inability to determine when a woman’s fertile window will close, testing can be done to predict how she will respond to medications used to stimulate her ovaries. These medications were initially used for in vitro fertilization (IVF) and are now being used for egg freezing, as well. The testing is called ovarian reserve testing and is generally done on day three of the menstrual cycle where day one is considered the first day of flow.
An ultrasound can be performed to look at the number of follicles within each ovary and calculate an antral follicle count- the total number of measurable follicles.
Blood can be drawn to test for follicle stimulating hormone (FSH), estradiol (E2), and anti-mullerian hormone (AMH). Follicle stimulating hormone is released from the brain and stimulates the ovary to develop follicles and the eggs within them. Estradiol is checked in conjunction with follicle stimulating hormone. It is produced from the ovary and it assists in the interpretation of follicle stimulating hormone levels. Anti-mullerian hormone is cycle independent, meaning that it can be checked at any time during the menstrual cycle. It is another marker used to estimate the pool of resting follicles within the ovary.
These tests are interpreted together to estimate a woman’s ovarian reserve. The tests do not predict a woman’s window of fertility nor is their utility in non-stimulated (IVF or egg freezing) settings fully understood at this time.
What is the preservation process like?
Patients who desire to have their eggs frozen will undergo a process called controlled ovarian hyperstimulation. This involves taking injectable medications on a daily basis to stimulate the ovaries to develop multiple follicles. The woman will be monitored with vaginal ultrasounds and blood tests until her developing follicles have grown adequately. At that time, the patient will be give herself a final injection, called the trigger shot, that helps prepare the eggs within the developing follicles for retrieval.
Approximately 36 hours after the trigger shot, the patient will have the eggs removed in a quick procedure and will be able to go home the same day. During the procedure, a physician uses ultrasound to find the woman’s ovaries and guides a needle into each developing follicle where the eggs are carefully removed. An embryologist identifies each egg, prepares it for freezing, and then freezes the egg. These eggs are frozen in time and will always reflect the woman’s age at the time they were frozen, not the age of the woman when it is thawed and used.
When a woman is ready to use her eggs, they are thawed, fertilized with sperm, and then transferred back into her uterus during a quick procedure called an embryo transfer.
Are there any long term effects of the process?
Research has shown that embryos created from egg donors where eggs are collected and frozen, then stored until desired use when they are thawed and fertilized, have equivalent outcomes to embryos from eggs that were not frozen prior to fertilization.[6] The potential of the frozen eggs to become a baby depends upon a woman’s age at the time of egg freezing, her ovarian reserve, and her health history. This will remain the same regardless of how long the eggs are frozen as they are essentially suspended in time.
The medications used have for egg freezing have been used for decades in the treatment of infertility with IVF and have not been shown to have long term risks. Additionally, babies born through IVF processes- which in most ways are the same as using frozen eggs- do not have an increased risk of birth defects or disorders above that that occurs with spontaneous pregnancies.
The egg freezing process does not decrease a woman’s egg supply. The medications she takes during the cycle rescue follicles that would otherwise die off when the primary follicle is selected and keep them alive to develop multiple useable eggs. The process does not steal eggs from future menstrual cycles.
Opinions from experts in the field
Increasing acceptance for egg freezing came in January of 2013 and January of 2014 when three well recognized fertility and OB/GYN societies (ASRM, SART, and ACOG) released statements that egg freezing should no longer be considered experimental.[7,8] The societies endorse the practice of egg freezing for patients undergoing gonadotoxic treatment.
They state that further evidence is required before recommending egg freezing specifically for use by patients who wish to electively defer childbearing as there is insufficient data to confirm its utility. This lack of data is primary a result of the newness of the technique and the small numbers of patients undergoing egg freezing previously.
Fertility preservation is catching on
Recently, egg freezing has become more mainstream in society, as well. Insurance companies are regularly covering the cost of fertility preservation for patients undergoing gonadotoxic therapies and now technological companies such as Facebook and Apple are paying for their employees to electively have their eggs frozen.
Some worry that this may be seen as encouraging women to delay childbearing and focus on their careers while others feel this is a liberating opportunity for women to uncouple reproduction from age. The long-term effects remain to be seen, but women who are interested should investigate the opportunity as well as their insurance coverage options.
As a woman in my 30’s who works in the field of reproductive endocrinology and who has seen the devastating impact of infertility I have chosen to electively freeze my eggs. I don’t now what the future holds for me, but I feel more secure knowing that I have placed my fertility on ice and not left it to chance.
References:
- Matthews, T and Hamilton, B. NCHS Data Brief No 152: First Births to Older Women Continue to Rise. May 2014.
- Sandalinas M, Marquez C, Munne S. Spectral karyotyping of fresh, non-inseminated oocytes. Mol Hum Reprod 2002;8:580-585.
- Pellestor F, Andreo B, Arnal F, Humaeu C, Demaille J. Maternal ageing and chromosomal abnormalities: new data drawn from in vitro unfertilized human oocytes. Hum Genet 2003;112:195-203.
- Fragouli E, Alfarawati S, Goodall NN, Sánchez-García JF, Colls P, Wells D. The cytogenetics of polar bodies: insights into female meiosis and the diagnosis of aneuploidy. Mol Hum Reprod 2011b;17:286-295.
- Fragouli E, Escalona A, Gutierrez-Mateo C, Tormasi S, Alfarawati S, Sepulveda S, Noriega L, Garcia J, Wells D, Munne S. Comparative genomic hybridization of oocytes and first polar bodies from young donors. RBM Online 2009;19:228-237.
- Sekhon et al. Frozen versus fresh donor egg IVF: similar efficacy and greater efficiency in a large donor egg IVF program. Fert Steril 2014;102(3):e83.
- ACOG: Committee Opinion No. 584: oocyte cryopreservation. Obstet Gynecol. 2014 Jan;123(1):221-2.
- Mature oocyte cryopreservation: a guideline. Practice Committees of American Society for Reproductive Medicine, Society for Assisted Reproductive Technology. Fertil Steril. 2013;99:37-43.
“We Thrive on the Cutting Edge”
Fluoroscopic Guided Procedures
Fluoroscopic (X-ray) guided procedures have become the standard of care in the treatment of spine injuries. Patient safety is assured with the use of high resolution imaging and expert physician skill. Dr. Christopher Rogers is a specialist in the performance of fluoroscopy (digital x-ray) guided spine and joint procedures. In 1996, he was the first Board Certified Physical Medicine and Rehabilitation physician in San Diego to have completed an Interventional Spine Care Fellowship. This program included advanced training with evidence-based methods in the diagnosis and treatment of spine pain. Since that time, he has treated more than 18,000 people with many different causes of lower back pain.
Diagnostic Musculoskeletal Ultrasound
Diagnostic Musculoskeletal Ultrasound uses high frequency sound waves to create digital images of tendons, ligaments, cartilage, muscles and nerves. This procedure provides resolution that is up to ten times that of magnetic resonance imaging (MRI). The exam is performed in the office while the patient is able to observe the results in real time. The use of ultrasound guidance allows the precise, safe and comfortable injection of orthobiologics such as platelets or regenerative stem cells.
Dr. Christopher Rogers is an expert in the use of diagnostic musculoskeletal ultrasound and ultrasound guided therapy. He has trained hundreds of physicians in the use of diagnostic ultrasound and has performed thousands of ultrasound guided procedures.
Platelet-Rich Plasma (PRP) Therapy
In 2009, Dr. Rogers became one of the first physicians in San Diego to successfully treat a patient with an elbow injury by utilizing platelet-rich plasma (PRP) therapy. It is used to treat such conditions such as tendon, ligament, muscle, and nerve injuries, and joint arthritis. Dr. Rogers has performed more than one thousand ultrasound-guided PRP treatments and has trained dozens of physicians in the appropriate use of PRP therapy.
ENDORET (PRGF) Technology
Dr. Rogers was the first physician in San Diego (and the third in the United States) to treat a patient with a tendon injury using the ENDORET plasma rich growth factor (PRGF) therapy.
Endoret (PRGF) technology uses a clinically proven Platelet-Rich Plasma Processing System to produce more rapid healing and decreased pain. It is safe and versatile, with clinical efficiency in tissue healing and regeneration.
Lipogems Therapy
Lipogems is an FDA approved medical device used for the treatment of tendon, ligament and joint injuries. It uses the body’s own fat tissue to cushion and support injuries for rapid and effective healing. It is a very good option for patients wishing to avoid a total knee or total shoulder joint surgery.
Dr. Rogers is a pioneer in the use of Lipogems in the United States. He was the first physician in San Diego to successfully treat a patient with knee arthritis using Lipogems therapy. In addition, he trains physicians from around the world at The Orthobiologic Institute (TOBI) training course each year.
Bone Marrow Concentrate (BMC) Therapy
Bone marrow is known to contain a variety of cells that stimulate the healing of tendon, ligament and joint injuries. Bone Marrow Aspirate Concentrate (BMAC) Therapy is a scientifically proven regenerative medicine therapy used for the rapid healing of moderate to severe arthritis and tendon injuries. With our advanced bone marrow harvesting procedures, we produce a more viable and healthy cellular based treatment. In our state-of-the-art lab, the harvested bone marrow cells are analyzed with flow cytometry cell counters prior to treatment in order to customize and optimize our treatment results.
Pulsed Electromagnetic Therapy (PEMF)
Pulsed Electromagnetic Field Therapy is a pain-free and safe method that has been used in Europe for more than two decades. This therapy has been shown in prospective clinical trials to reduce the pain and inflammation of joint arthritis. It improves systemic microcirculation, cellular detoxification, and the regeneration of bone, tendon and cartilage. It has also been proven to improve energy and decrease fatigue.
MyBioProfile
San Diego Orthobiologics Medical Group physicians recognize that each person is unique. The MyBioProfile Evaluation is a comprehensive evaluation that considers each person’s unique regenerative capacity by analysis of your anatomy, biomechanics and cellular biochemistry. This evaluation allows your team of doctors to modify and customize your treatment plan to ensure optimal and long lasting results.
Virtusense 3D Motion Analysis
Virtusense 3D motion Analysis is an advanced method of motion capture of your entire musculoskeletal system. It uses laser tracking without any sensors on the body, plus it is safe for the eyes. Different movements such as bending, squatting, lunges, joint mobility and rotary stability are monitored to measure treatment improvements and sports performance.
While other medical clinics simply focus on your symptomatic joint, the San Diego Orthobiologics Medical Group uses motion analysis to understand how your injury relates to the other joints in your body. Extremely precise measurement of movement restrictions and muscle imbalances can identify risk factors for a repeat injury.
Advanced Laboratory Testing
Your comprehensive evaluation will include advanced laboratory testing of micronutrients, systemic inflammation and biomarkers of regenerative potential. This allows your physician to make customized dietary and supplement recommendations to enhance your response to Regenerative Medicine Therapies.
Summary
Our facility has some of the most advanced Regenerative Medicine technologies available in San Diego. We provide many diagnostic tests and advanced Regenerative Medicine not available at any other clinic. Every treatment is performed by a board certified Regenerative Medicine physician with advanced ultrasound or fluoroscopic imaging training. We look forward to seeing you soon at the San Diego Orthobiologics Medical Group where customized care and excellent results are our top priority.
Sharp Mary Birch Education Center
Sharp Mary Birch now has offerings in North County! The Sharp Mary Birch Education Center in Carlsbad includes physician offices and an education space where the hospital will host classes such as Childbirth Preparation, Baby Care Basics, and Breastfeeding.
Childbirth Preparation One-Day Class
This class is designed for busy couples who want the basic facts about childbirth preparation in one day.
Saturday, May 12, 2018
9:30 AM to 4:00 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
Saturday, June 9, 2018
9:30 AM to 4:00 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
Childbirth Preparation Four-Week Class
Our popular childbirth preparation classes prepares expecting parents for everything from labor and delivery to breastfeeding and newborn care.
Begins Tuesday, May 15, 2018
6:30 PM to 9 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
Begins Tuesday, June 26, 2018
6:30 PM to 9 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
Baby Care Basics Class
In this hands-on class, parents learn all the basic baby care they need to know
before heading home with their newborn, including diapering, dressing,
swaddling and more.
Saturday, May 26, 2018
9:30 AM to 12 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte
Carlsbad, CA 92011
More info
Tuesday, June 12, 2018
6:30 PM to 9:00 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte
Carlsbad, CA 92011
More info
Friday, June 15, 2018
9:30 AM to 12:00 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte
Carlsbad, CA 92011
More info
Breastfeeding Class
This class teaches the basic skills for successful breastfeeding so parents can feel more comfortable and confident once their baby arrives. Topics include positioning, proper latch, breast pumps, and more.
Saturday, May 26, 2018
12:30 to 3:30 pm
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte
Carlsbad, CA 92011
More info
Friday, June 15, 2018
12:30 to 3:30 pm
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
Tuesday, July 24, 2018
6:30 PM to 9:30 PM
Offered by: Sharp Mary Birch Hospital
Where: Sharp Mary Birch Education Center
6125 Paseo Del Norte, Suite 130
Carlsbad, CA 92011
More info
For more on classes, click here.
Many transgender individuals are of reproductive age at the time of transition, so it is imperative that family-building goals are part of the conversation. Though not exhaustive, this post is designed to help transgender individuals understand their fertility options and barriers they may encounter at different points in transition. Regardless, transgender individuals should speak to a fertility specialist (called a Reproductive Endocrinologist) to discuss the impact of hormonal and/or surgical treatment on their fertility, as well as options for fertility preservation. They should also speak with an experienced counselor to help address the potential impact of fertility treatments on any gender dysphoria, the impact of temporary discontinuation of hormonal therapy and the need for emotional support.
*For the purposes of this article, to avoid confusion, transitioning males will be referred to as FTM and transitioning females will be referred to as MTF.
Prior to Hormone Therapy and/or Surgery
For FTM individuals, improvements in cryopreservation (freezing) technology have made freezing eggs a realistic option for many. To do so, a series of injections of ovarian stimulating hormones are given for ~10-12 days, with frequent monitoring with ultrasound and estrogen levels. When the eggs are ready for retrieval, a transvaginal egg retrieval is performed under light anesthesia, using a small needle that punctures through the vaginal wall and into each ovary. Risks related to the medications and the egg retrieval procedure are minimal. Recovery is quick, with most people able to return to work or school the next day. Eggs are frozen on the day of retrieval and remain in cryopreservation until ready for use. Long-term viability and utility of eggs is still unknown as the freezing technology is still relatively new. The number and quality of eggs available for retrieval is best in younger individuals, optimally ≤ 30 years old. Prior to treatment, an assessment of quantity can be made to tailor expectations for egg retrieval. Though still experimental, cryopreservation of ovarian tissue at the time of hysterectomy can also be considered. This is currently only performed at specifically designated research sites under institutional review board (IRB) approval.
For MTF individuals, sperm tend to be very robust and survive freezing for extended periods of time. For this reason, sperm cryopreservation is an excellent option for potential use in the future, either for inseminations (IUI) or with more advanced technology like in-vitro fertilization (IVF). A number of collections (usually 4-6) is recommended to increase options for use.
After Hormone Therapy
Reproduction for transgender individuals who have initiated transition with hormones will typically involve temporary discontinuation. This can cause difficult physical and emotional changes that are best addressed actively with a qualified mental health professional as part of the treatment process.
The impact of long-term hormone exposure on eggs, sperm and offspring is essential unknown. It is imperative that individuals who choose to pursue treatment understand the limitations of our current knowledge.
For FTM, several options exist. For individuals wishing to carry a child, case reports[1] have shown spontaneous resumption of menses after discontinuation of testosterone therapy, even in situations of use for many years. In another study[2], 57% of individuals had been on hormone therapy for an average of 3.7 years. However, 23% required the assistance of a fertility specialist to conceive, suggesting that the previous testosterone exposure may have affected the function of the ovary. For individuals wishing to preserve eggs, case reports[3] also exist showing successful egg retrieval. Protocols were even used to minimize negative impact of estrogen exposure, improving patient compliance.
For MTF, most data regarding resumption of sperm production after sex steroid suppression comes from short-term male contraception studies; this means the data is not necessarily applicable to the transgender population who are using estrogen, particularly for long periods of time.[4] The data we do have would suggest that return of sperm production is slow (many months), and sometimes not at all. Therapies are available to promote resumption of sperm production; these can be discussed with a Urologist who specializes in fertility or a Reproductive Endocrinologist.
Non-Biological Options
For transgender individuals who have had surgery or do not wish to disrupt their hormone therapy, many options still exist for family building. Egg and sperm donors (from known or anonymous sources) as well as gestational carriers can be part of a family building plan.
For transgender individuals interested in family planning, it is critical that they are informed of their options. Because there are currently no formal practice guidelines for physicians providing fertility guidance and care to transgender individuals, it is important to make sure you seek advice from experts in the field of Reproductive Endocrinology and/or Urology. These specialists can help guide you through options, risks, and outcomes to optimize your care.
Best Wishes in Reproductive Health!
Wendy B. Shelly, MD
Board Certified, Obstetrics/Gynecology and Reproductive Endocrinology
Fertility Specialists Medical Group
[1] Gidoni YS, Raziel A, Strassburger D, Kasterstein E, Ben-Ami I, Ron-El R. Can we preserve fertility in a female to male transgender after a long term testosterone treatment – case report. Fertil Steril 2013;100:P-77.
[2] Light AD, Sevelius J, Obedin-Maliver J, Kerns J. Pregnancy after transitioning: the male-gendered experience with fertility, pregnancy, and birth outcomes. Fertil Steril 2013;100:P-895.
[3] Rodriquez-Wallberg KA, Dhejne C, Stefenson M, Degerblad M, Olofsson JI. Preserving eggs for men’s fertility. A pilot experience with fertility preservation for female-to-male transsexuals in Sweden. Fertil Steril 2014;102:P-65.
[4] Stahl P. Recovery of spermatogenesis after hormone therapy: what to expect and when to expect it. Fertil Steril 2017;107:338-339.
San Diego Orthobiologics Medical Group is pleased to have been the first medical center in San Diego to offer the revolutionary LIPOGEMS® Regenerative Medicine therapy.
LIPOGEMS® is an FDA approved medical device used to process regenerative cells derived from your own fat tissue. It’s used for the treatment of joint pain and tendon injuries.
Why is the LIPOGEMS® treatment so unique?
Lipogems is a game changer in Regenerative Medicine due to its cutting edge technology that uses your body’s own fat tissue to cushion and support injured areas as your body heals itself. Lipogems is an FDA-cleared medical device that is used to harvest, concentrate, and transfer autologous (your own cells) adipose tissue. The adipose tissue that is being processed by Lipogems is ‘minimally manipulated’ in accordance with FDA’s criteria for human cell and tissue products. The fat tissue can be removed from the abdomen or thigh areas. This tissue is then precisely injected into the patient’s injured areas with the use of ultrasound or x-ray guidance.
Unlike steroid or gel injections, the tissue will stay in the treated area for years allowing your body to maximize the benefits for an extended period of time. The Lipogems procedure can be performed in less than one hour in an outpatient clinical setting.
Lipogems was awarded Best New Technology in Sports Medicine in 2016 by Leading Sports Medicine Physicians.
LIPOGEMS® is a comprehensive Regenerative Medicine treatment that uses your own stem cells and their cellular ‘niche’ to maximize results. Mesenchymal stem cells require support from other cells and proteins to exert their healing benefits. Unlike other so-called ‘stem cell’ treatments, the unique advantage of LIPOGEMS® is that the complete healing environment of the fat tissue is maintained to improve cell viability and regenerative capacity.
Dissolving the fat with enzymes as occurs with stromal vascular fraction (SVF), eliminates or destroys some of stem cells and tissues required for healing. This activity is prohibited by the US Food and Drug Administration (FDA) without special permission or research licenses.
What are the Practical and Scientific Benefits of Adipose Tissue?
- Research has shown that regardless of a person’s age, their fat maintains certain reparative properties unlike other tissues such as bone marrow, which may lose healing capacity with age.
- Minimally invasive and pain-less procedure
- Abundant number of cells unlike bone marrow or amniotic tissue
- Contains high concentration of micro-vessels which harbor specialized healing cells such as perivascular cells, also called pericytes
What is the Lipogems® device?
The Lipogems® device is a class II A sterile medical device intended for the closed-loop processing of your own fat tissue in medical procedures involving the harvesting, concentrating and transferring of a patient’s own adipose tissue. It gently washes inflammatory impurities from the adipose tissue using saline and resizes the adipose tissue to create an optimal size to inject the Lipogems precisely into desired tissue locations by the physician.
Am I a candidate for Lipogems therapy?
Lipogems has now been successfully performed in more than 8,000 clinical cases globally.
You are a candidate if you:
- Suffer from an injury or condition that limits your normal daily functioning due to a soft tissue defect in the tendon, ligament, muscle or joint cartilage.
- Treatment options, such as physical therapy, medications or steroid injections have not provided permanent relief.
- You would like to consider alternatives to a total hip, shoulder or knee joint replacement surgery.
- You do not suffer from a severe medical illness (cancer, infection, bleeding disorder), are pregnant or breastfeeding, or unable to temporarily discontinue blood thinner medications.
Lipogems® Testimonials
Patients undergoing the Lipogems procedure at our clinic undergo a strict screening procedure to assure that they are ideal candidates for the treatment.
Within the last 23 months of tracking our outcomes, more than 90% of our patients experienced significant relief with the treatment and were reported to resume normal, pain- free physical activity. Most of our patients have been able to improve their fitness, lose weight and improve the quality of their lives in a meaningful way.
San Diego Orthobiologics Medical Group is very excited to offer this Regenerative Medicine to our patients, while conducting ongoing clinical research in improving patient care and comfort.
July 6, 2017
Dear Fertility Specialists Medical Group in San Diego,
How can I check how many eggs I have left?
Thanks!
Sarah
Hi Sarah,
Thank you for your important question. At Fertility Specialists Medical Group in San Diego we get this question all of the time. Our current understanding is that women are born with every egg they will ever have. This means that, over time, your supply decreases and, therefore, age is a major predictor of fertility .
One of the best determinants of egg supply is an ultrasound that looks at the ovaries. During the ultrasound there are black circles or follicles that are seen on the ovaries. These follicles have zero or one developing egg within them. Your doctor will count the total number of follicles on each ovary and add them to get your Antral Follicle Count. This number is the first estimate of your egg supply. An ultrasound is included in your initial consult at Fertility Specialists Medical Group in San Diego. This number is not your total egg supply, but a representation of that supply. The majority of your eggs are actually in a quiet resting state and are too small to be seen on an ultrasound. Each month a percentage of them wake up and become responsive to signals from the brain and start to grow. These growing follicles are what we see on ultrasound. We use this number, in conjunction with blood tests, to estimate your egg supply. You won’t get an exact number of eggs you have, but a category such as good, medium, or low. The blood tests we use are: Anti-Mullerian Hormone (AMH), an Ovarian Assessment Report (OAR), and/or Follicle Stimulating Hormone (FSH) in conjunction with Estradiol (E2).
At Fertility Specialists Medical Group in San Diego we will review your history and discuss which of these tests are appropriate for you. In general, the higher your levels of AMH the higher your egg supply is. This is because AMH is released from the follicles that are seen on your ultrasound. So, the more follicles you have, the more AMH you have. Conversely, the higher your FSH, the lower your egg supply. That is because FSH is your brain’s volume nob for talking to the ovary and asking it to produce an egg. The lower your egg supply is the louder your brain has to talk to your ovaries (higher FSH) to produce an egg. The OAR is a computational algorithm that takes in to account your AMH, FSH, and E2 along with the other hormones: Inhibin (InhB) and Luteinizing Hormone (LH) as well as your age. The advantage of this test is that it can roughly predict how many eggs you would have with an IVF or egg freeze cycle.
I know this is a lot of information, Sarah, but the basics are that you have an ultrasound and blood tests to determine your ovarian reserve.
If you are interested in learning more about what testing would be right for you please come visit us at Fertility Specialists Medical Group in San Diego. As three female physicians’ deeply committed to helping women learn more about their reproductive health and take control of their own reproductive timeline we offer complementary egg freezing consults at Fertility Specialists Medical Group in San Diego.
Sincerely,
 Dr. Maas
Dr. Maas
Fertility Specialists Medical Group
San Diego, CA
Carlsbad, CA
![]()